A cirrhosis diagnosis often triggers one urgent question: how serious is it? That question makes sense, because cirrhosis is not a single fixed state. It is a spectrum. Some people have cirrhosis that is present but still relatively stable. Others have cirrhosis with major complications such as fluid buildup, internal bleeding, confusion, or liver failure.
That difference matters. It affects symptoms, prognosis, surveillance, treatment decisions, and whether transplant evaluation becomes part of the conversation.
This guide explains the stages of cirrhosis in plain language, including compensated cirrhosis, decompensated cirrhosis, common complications, what affects prognosis, and how patients are monitored over time.
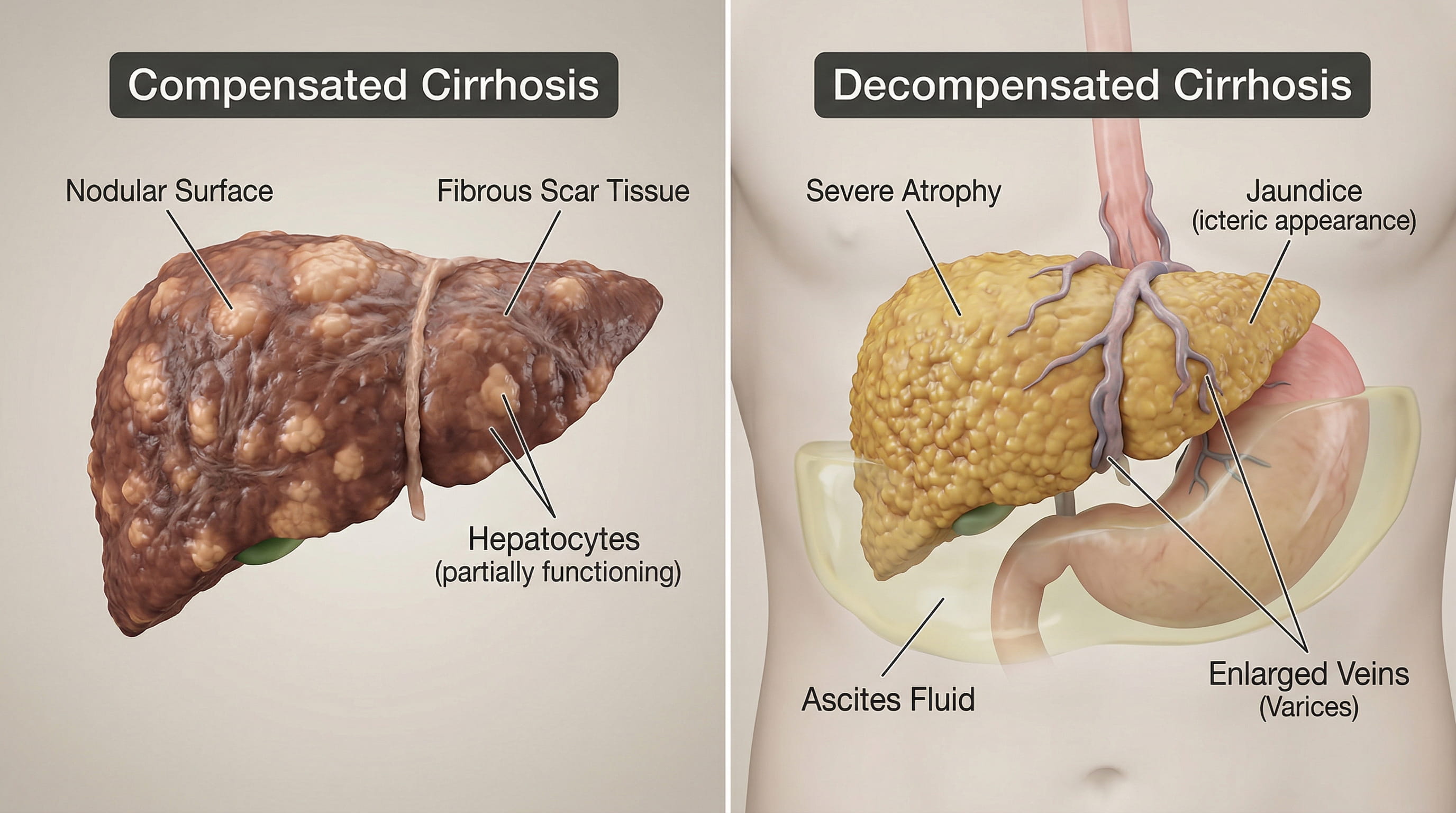
Cirrhosis is commonly discussed in two broad stages: compensated and decompensated.
Compensated cirrhosis means the liver is scarred but still able to perform enough of its essential functions that major complications have not yet developed.
Decompensated cirrhosis means complications have started. These complications may include ascites, variceal bleeding, jaundice, hepatic encephalopathy, or recurrent infections.
The shift from compensated to decompensated cirrhosis is one of the most important turning points in liver disease care.
Compensated cirrhosis refers to a stage in which the liver has significant scarring, but the body is still coping well enough that obvious complications are absent or limited.
A person with compensated cirrhosis may:
This stage is serious, but it is often the best time to intervene aggressively. Treating the underlying cause, avoiding alcohol, controlling metabolic risk factors, and monitoring for complications can slow progression.
Decompensated cirrhosis means the liver and the circulation around it can no longer compensate for the scarring. At that point, complications begin to appear.
Major signs of decompensation include:
Once a person becomes decompensated, care becomes more complex and close follow-up is essential.
The liver responds to chronic injury by laying down scar tissue. Over time, that scar tissue changes the liver’s structure and interferes with blood flow through the organ. This increases pressure in the portal vein system, a problem known as portal hypertension.
Portal hypertension is a key reason cirrhosis becomes dangerous. It contributes to fluid buildup, enlarged veins in the esophagus or stomach, splenomegaly, low platelets, and bleeding risk.
Ascites is the buildup of fluid in the abdomen. It is one of the most common signs that compensated cirrhosis has become decompensated.
Patients may notice:
Ascites increases the risk of infection and often requires sodium restriction, diuretics, and sometimes drainage procedures.
When portal pressure rises, blood looks for alternate pathways around the liver. This can create fragile enlarged veins called varices, especially in the esophagus and stomach.
If varices rupture, they may cause:
This is why screening endoscopy and portal hypertension management matter in cirrhosis care.
Hepatic encephalopathy happens when the diseased liver cannot clear toxins effectively. Those toxins can affect brain function.
Symptoms may include:
This can range from subtle brain fog to severe mental status changes. New confusion in a cirrhosis patient is always important.
Jaundice happens when bilirubin builds up in the body. It causes yellowing of the skin and eyes and may be associated with dark urine and pale stools.
Jaundice often signals worsening liver function or bile flow problems and is an important marker of disease progression.
People with cirrhosis are more vulnerable to infections, especially when ascites is present. Fever, abdominal pain, worsening confusion, or sudden illness can signal infection and need prompt evaluation.
Advanced cirrhosis can affect kidney function through changes in circulation, inflammation, and fluid balance. This increases overall risk and can complicate treatment.
Cirrhosis is one of the most important risk factors for hepatocellular carcinoma. That is why ongoing screening is part of routine cirrhosis care.
Patients often search for “cirrhosis life expectancy,” but there is no single timeline that fits every person. Prognosis depends on multiple factors, including:
That means two people with the same diagnosis may have very different clinical courses.
Doctors use symptoms, exam findings, labs, imaging, and scoring systems to understand how advanced cirrhosis is.
This system helps estimate severity based on bilirubin, albumin, clotting, ascites, and encephalopathy.
The MELD score is widely used to estimate disease severity and help determine transplant priority.
Ultrasound, CT, MRI, elastography, and upper endoscopy help identify portal hypertension, varices, nodular liver changes, splenomegaly, ascites, and liver masses.
Some patients feel reassured when they hear the word “compensated.” That is understandable, but compensated cirrhosis still requires serious follow-up.
Why? Because the liver is already scarred. A person may feel well today but still have ongoing injury, portal hypertension, or a rising risk of cancer and future decompensation. The goal at this stage is not to wait for symptoms. It is to prevent them.
Yes. Some patients remain stable for long periods, but cirrhosis can also worsen quickly after bleeding, infection, alcohol use, medication injury, hepatitis flare, or kidney problems.
That is why regular follow-up matters even when symptoms are mild.
Good cirrhosis care usually includes:
Surveillance is not optional in cirrhosis. It is part of preventing avoidable complications.
A liver transplant is not the first step for every person with cirrhosis, but it becomes more relevant when the disease is advanced, complications recur, or liver function continues to worsen despite treatment.
Transplant discussions often arise with:
A new cirrhosis diagnosis should prompt clear questions, such as:
These questions lead to better next-step planning and more informed long-term care.
Cirrhosis stage matters because it changes what the diagnosis means in real life. Compensated cirrhosis means the liver is scarred but has not yet triggered major complications. Decompensated cirrhosis means the complications have started and the risks are higher.
The earlier cirrhosis is identified and managed, the better the chance of slowing progression, preventing hospitalizations, and preserving quality of life. For patients who need digestive or liver-related evaluation, GastroDoxs can help initiate the workup and guide next-step GI care.
Many patients search for terms like “stage 1 cirrhosis” or “stage 4 cirrhosis.” Online, cirrhosis is sometimes described in four stages, but in real clinical practice the more meaningful distinction is usually compensated versus decompensated disease.
That said, the four-stage language is often used in a simplified way:
This type of staging can be useful for patient education, but it is less precise than the systems doctors actually use for management and prognosis.
The first major complication changes the whole conversation. A patient who has never had ascites, bleeding, or encephalopathy is managed very differently from someone who has already had one of those events.
After the first decompensating event, doctors watch more closely for recurrence, infection, hospitalizations, nutrition decline, kidney injury, and need for transplant referral. This is why the appearance of new ascites or a bleeding episode is not just another symptom. It is a meaningful shift in disease course.
Not every hospital stay means liver failure, but hospitalization in cirrhosis should never be ignored. Common reasons include gastrointestinal bleeding, infected ascites, severe encephalopathy, worsening jaundice, kidney dysfunction, and rapid fluid accumulation.
For some patients, a hospital stay becomes the moment when cirrhosis is first recognized. For others, it signals that previously compensated disease has become unstable.
Patients often focus only on bilirubin or liver enzymes, but nutrition is also important. Muscle wasting and frailty are common in cirrhosis and can meaningfully affect resilience, mobility, infection risk, recovery after complications, and overall outcomes.
That is why weight alone can be misleading. A person may appear stable or even heavier because of ascites, while actually losing functional muscle mass underneath.
Yes, some people with compensated cirrhosis live for years with careful monitoring and treatment of the underlying cause. Others progress more quickly because of bleeding, infection, ongoing alcohol use, liver cancer, kidney problems, or severe portal hypertension.
The key point is that prognosis is dynamic, not fixed. It can improve or worsen depending on what happens after diagnosis and whether complications are prevented or controlled.
Two people may both have cirrhosis, but the underlying reason still matters. A patient who stops alcohol completely, controls metabolic risk factors, and adheres to surveillance may do much better than someone whose liver continues to be injured. Likewise, a patient with controlled viral hepatitis may have a different trajectory than someone with recurrent untreated inflammation.
That is why every cirrhosis workup should answer not only “how advanced is it?” but also “why did it happen?”

Symptoms between visits often tell the real story. Families should watch for:
These changes can signal worsening decompensation and should prompt medical guidance quickly.
Dr. Bharat Pothuri is a Board-Certified Gastroenterologist and Hepatologist. With extensive experience in digestive health, he specializes in advanced endoscopic procedures, chronic GI disorder management, and preventive care. Dr. Pothuri is dedicated to providing expert, patient-focused insights to help improve gut health and overall well-being.
Compensated cirrhosis means the liver is scarred but major complications have not yet developed. Decompensated cirrhosis means complications such as ascites, bleeding, jaundice, or encephalopathy have appeared.
Yes. It is often more stable than decompensated disease, but it still requires treatment, monitoring, and surveillance.
Some complications can be controlled, and liver function may improve when the cause is treated, but advanced cirrhosis remains a serious condition.
Not always immediately, but ongoing injury and complications increase that risk over time.
Transplant is usually considered when cirrhosis becomes advanced, repeatedly decompensates, or leads to high-risk complications.